Medical and Surgical Gastroenterology Hospitals India
Prevention, diagnosis and treatment of diseases of the digestive tract, liver and pancreatico-biliary system in children and adults is the core objective of the Centre of Medical and Surgical Gastroenterology at We Care India partner Hospitals India. The hospitals offer state of art endoscopic procedures for gastrointestinal bleed, gastrointestinal cancers, foreign bodies, obstructive jaundice, pancreatitis and feeding techniques. It has provisions for MARS and all facilities for various modalities of treating liver cancer like surgery, RFA, chemoembolisation and percutaneous injections are available.
The gastrointestinal surgeons manage major gastro-intestinal surgical problems of the intestines, pancreas and hepatobiliary tract including cancers, many of them through minimal access surgery.
The Hepatologists and transplant surgeons at We Care partner Hospitals in India work as a team and have established India's first Liver Centre. It is equipped with high-end technology to perform precise surgery in this newly developed modality of surgical treatment. Living donor and cadaveric liver transplant are both performed in children as well as adults. With more than a 150 livers transplanted in the years gone by, we now perform 8 -10 liver transplants every month with world comparable success rates.
Highlights of the center of Gastroenterology Surgery at Hospital in India
Comprehensive specialty care for diseases of the liver, pancreas and bile duct including Liver transplants.
Treatment of major gastrointestinal surgical problems - including cancers, hepatobiliary and pancreatic diseases.
Routinely performs Colorectal Surgery , Minimal Access Surgery ,Bariatric Surgery and Diagnostic & Therapeutic Endoscopies.
Constantly involved in major research programs at the basic, applied, and translational levels to generate new knowledge that ultimately benefits patients.
Gastrointestinal Surgery
Major surgeries for benign and malignant conditions of oesophagus, stomach, intestines, liver and pancreas are carried out routinely. Minimally invasive Cholecystectomy, Appendectomy, Splenectomy and Intestinal Resections are also routinely performed. Surgery for Hiatus Hernia is another commonly performed procedure.
The other specialty of the centre of Gastrointestinal Surgery at We Care partner hospital is that complex Biliary reconstruction surgery for bile duct strictures is performed on par with any other centre in the world with excellent results.
The Minimally Invasive Surgery Division at We Care partner hospital in India is one of the centers performing the largest number of laparoscopic procedures in the country, performing not only basic laparoscopic procedures but also most of the advanced laparoscopic procedures like laparoscopic esophageal surgery, gastric resections, colorectal surgery, pancreatic surgery and small bowel surgery. We have a state of the art Aida Touchscreen facility, and DVD recording facility and a newer version of the Harmonic Scalpel for bloodless surgery.
Liver Transplants
The Center for Liver Diseases and Transplantation at We Care India partner hospitals in India is equipped with the state-of-the-art technology for liver surgery using the laparoscopic Argon Beam Laser as well as Tissue Link in combination with other methods of liver resection like CUSA and Laparoscopic Vascular Stapling. Bloodless Liver Surgery is performed with high success rates.
Who is eligible for liver transplant at hospital in India ?
While a liver transplant is the best cure for most patients with non-metastatic liver cancer, the limited organ supply may make this option unviable. The eligibility criteria for transplantation is the presence of a single HCC tumor 5 cm or less in diameter, or fewer tumor nodules, each 3 cm or less in diameter. Both living relative and cadaveric liver transplants are options for patients at the Center for Liver Diseases & Transplantation, We Care partner Hospitals in India. Patients who will obtain maximum benefit from liver transplantation include those who are estimated to have less than one to two years of life and have no alternative medical or surgical therapies. The liver transplant procedure helps prolong the patient's life for at least five years and/or to restore the patient to a normal or near normal functional status. Thus, the overall goals of liver transplantation are to prolong life and improve the quality of life.
What are the conditions for which liver transplant is done at hospital in India ?
Irreversible cirrhosis with at least two signs of liver insufficiency
Fulminant hepatic failure: coma - Grade 2
Unresectable hepatic malignancy that is less than 5 cm in diameter and confined to the liver
Metabolic liver disease that can be treated by liver replacement
MELD score of 12 or higher
Other specific indications for liver transplantation include Budd-Chiari Syndrome, benign hepatic tumor and autoimmune liver diseases. In addition, there should be no alternative forms of therapy and no contraindications for the procedure. Finally, the patient and family members should be able to accept the procedure and provide for its costs.
The most common indication for liver transplantation however is end-stage chronic liver disease, accounting for approximately two-thirds of all patients.
General clinical and biochemical indications for liver transplantation in patients with chronic cholestatic liver diseases (e.g., primary biliary cirrhosis and primary sclerosing cholangitis) include : -
>> Serum bilirubin > 8-10 mg/dL
>> Intractable Pruritus
>> Intractable bone disease
>> Malnutrition or recurrent bacterial cholangitis
>> Severe or intractable encephalopathy
In patients with chronic hepatocellular diseases (e.g., chronic hepatitis with cirrhosis), general biochemical indications for liver transplantation include : -
>> Serum albumin < 3.5 g/dL
>> Prothrombin time > 3 seconds above control or INR >1.3
>> Encephalopathy
>> Ascites
>> Bilirubin > 2 mg/dL
Patient Selection for Liver Transplantation
Minimum Listing Criteria for Liver Transplantation
CTP score > 7 (CTP Grade B)
MELD = 12
Life expectancy < 85% at 1 year without liver transplantation
Evidence of Clinical Decompensation in Chronic Liver Disease
In all/any category of advanced liver disease, the following conditions necessitate liver transplantation without further delay since they are associated with a very high incidence of life threatening complications : -
Intolerance to diuretics (low serum sodium/elevated kidney functions)
Recurrent or severe hepatic encephalopathy
Spontaneous bacterial peritonitis
Hepatorenal syndrome
Development of small hepatocellular carcinoma seen by liver imaging (CT Scan/Ultrasound)
Contraindications to Transplant
Contraindications to liver transplantation can be divided into those that are absolute and those that are relative, i.e., are expected to complicate and increase the risk of transplantation.
Absolute contraindications to liver transplantation include : -
AIDS or HIV positivity
Irreversible brain damage
Multi-system failure that is not correctable by liver transplantation
Malignancy outside the liver (except skin cancer)
Infection outside the hepatobiliary system
Active alcohol or substance abuse
Advanced cardiopulmonary or other systemic disease
Moderate to severe uncorrectable pulmonary artery hypertension
Completely occluded porto-mesenteric venous system
Factors that increase the risk of liver transplantation include the following : -
Advanced age
Advanced chronic renal failure
Cholangiocarcinoma
Chronic Hepatitis B virus infection with high viral counts
Hepatocellular carcinoma beyond Milan Criteria
Hypoxemia from intrapulmonary shunts
Massive ascites
Portal vein thrombosis
Prior portosystemic shunt surgery
Prior biliary tract surgery
Severe malnutrition
Severe abdominal atherosclerosis
The Liver Transplant team at We Care Partner Hospitals in India uses the above general principles as well as prognostic indices that are under development for conditions such as fulminant hepatic failure, primary biliary cirrhosis and primary sclerosing cholangitis. Early referral for pre-operative evaluation for liver transplantation is critical and allows evaluation before the development of multiple or advanced complications, which decrease the survival and increase the costs of liver transplantation.
Early referral allows close follow-up of patients with end-stage liver disease with the referring physician and an adjustment of priority status for transplantation. In addition, the family members and patient have ongoing education regarding the liver transplant process.
How is a patient evaluated prior to liver transplant at hospital in India ?
The majority of pre-transplant evaluations can be completed on an outpatient basis over a two-three day period. Candidates for transplantation are typically seen by the transplant surgeon, transplant hepatologist, transplant nurse coordinator, psychiatrist, nutritionist/dietitian, financial counselor and other consultants as appropriate.
(Consultations/consults for cardiology, pulmonary, oncology, etc. are performed by specialty physicians at Apollo Hospitals, who have expertise in working with patients with end-stage liver disease and organ complications/interactions from other systems. These consultations by our physicians are necessary for subsequent patient listing and transplantation). The transplant coordinator is the key contact person who facilitates the pre-transplant evaluation.
Transplant candidates over the age of 55-60 years or candidates over the age of 50 with risk factors for coronary disease, or those with a history of cardiac disease, undergo cardiology consultation with appropriate cardiac studies, often including stress thallium and/or cardiac catheterization. Doppler of carotid or peripheral vessels may also be appropriate. Cancer screening as per standard recommendations (Pap smear, mammogram, fecal occult blood testing, and flexible sigmoidoscopy depending upon age/gender), is completed.
Once the pre-transplant evaluation is completed, the patients profile is presented to the selection committee for categorization and prioritization
Patients are generally assigned to one of four categories : -
Suitable and ready, with listing and initiation of donor search
Suitable but too well, with placement on inactive status and followed with consultation with physician
Potentially reversible current contraindication, with treatment and recategorization at a later date
Irreversible absolute contraindication with denial of transplantation
Transplant options for alcoholic cirrhosis
There are a number of specific indications and/or circumstances regarding liver transplantation that undergo special scrutiny. One of these conditions is alcoholic cirrhosis. Apollos experience, as well as that of other transplant centers, has indicated that properly selected patients with alcoholic cirrhosis experience excellent survival and good quality of life following liver transplantation.
All patients referred to We Care partner hospitals in India undergo careful evaluation by a hepatologist, psychiatrist and social worker with attention to indicators for continued sobriety and compliance with the post-transplant long-term follow up. In particular, previous social stability, employment record, psychiatric status and length of sobriety are evaluated. For patients with the diagnosis of alcohol dependence or abuse, the referring physician will ask the patient to sign an alcohol contract and participate in alcohol recovery while awaiting transplantation. Only patients having psychosocial factors predicting long-term sobriety are accepted for transplantation.
Transplant options for chronic Hepatitis B Virus (HBV) Infection
Patients who have chronic Hepatitis B Virus (HBV) Infection are a subset of patients who present a special problem because of recurrent infection of the transplanted organ. Based on encouraging results from a number of European and US centers, we are currently treating all patients with Lamivudine & Hepatitis B Immune Globulin (HBIG) (selective) post-transplant in an attempt to reduce the rate of recurrence of infection in the allograft (now less than 10%). We are currently accepting patients with chronic HBV infection whether they are HBeAg/HBV DNA negative or positive. We also use lower doses of immunosuppressive medications post-transplant in hopes of reducing clinically significant HBV infection.
Liver transplants in older patients
Older patients also undergo special scrutiny. All candidates referred for liver transplantation past the age of 60 undergo particularly thorough evaluation, with particular attention to silent coronary or vascular disease. If patients have no other major organ disease and are expected to live five or more years, they are typically approved for transplantation.
Liver transplants for patients with hepatocellular carcinoma
Patients with hepatocellular carcinoma undergo special scrutiny and adjunctive therapy. They have a long-term survival after liver transplantation, which is less than that for patients undergoing transplantation for other indications. In order to improve these results, we currently offer adjuvant therapy in the form of chemo-embolization or chemotherapy to control the spread of cancer cells or unrecognized micrometastases. All patients undergo thorough evaluation for identifiable malignancy outside of the liver, including chest CT scan, abdominal and pelvic CT scan & bone scan. Finally, the abdominal cavity is explored carefully at the time of transplantation before proceeding with the hepatectomy and transplantation.
Follow-up
All cases are followed-up for life with maintenance of master records under the Liver Transplant Program at Apollo Hospitals. Regular patient communication with liver transplant coordinators or transplant physicians and referring doctors is implemented to enhance the optimal long-term results.
Ablation (Radiofrequency or Cryoablation)
Patients who are not candidates for resection or transplantation due to inadequate liver reserve, large or multiple lesions in multiple lobes, fibrosis or cirrhosis can benefit from treatments such as CT-guided, laparoscopic or open radiofrequency or cryoablation.
With new radiofrequency (RF) ablation technology, liver tumors up to 7 cm in diameter can be treated. The ideal patient for RFA generally has no more than three lesions that are no greater than 5 cm (about 1.5 inches) in size.
RF ablation delivers radiofrequency energy to the tumor, heating it to high temperatures thereby destroying the lesion. During cryoablation, argon gas is delivered through probes inserted into the liver, creating an ice ball that freezes the tumor and destroys its cells.
Another option for patients who are not surgical candidates is PEIT, which involves the injection of alcohol into the tumor, causing immediate dehydration of the cytoplasm with consequent coagulation, necrosis and fibrous reaction. PEIT results in complete ablation in upto 75% of selected patients with hepatocellular carcinoma.
Hepatic Arterial Pumps
Indicated for patients with metastatic colon cancer, hepatic arterial pumps deliver chemotherapy to the liver through a catheter placed in the hepatic artery. The catheter is typically inserted via laparoscopic or open surgery and a pump, which delivers the chemotherapy, is implanted subcutaneously. The pump is generally filled with chemotherapy medication once a month.
Why Choose We Care partner Hospitals ?
With the use of advanced technology and surgical methods, patients now have more options than ever before for the treatment of hepatobiliary disease. We Care partner Hospitals in India for Liver Disease & Transplantation offers comprehensive specialty care for diseases of the liver, pancreas and bile duct. We emphasize on ongoing communication with referring physicians and incorporate them in the decision process of their patient's medical management. Following treatment, we follow up our care with an organized discharge report to the referring physician. Our physicians are trained at the worlds most renowned centers in Hepatobiliary surgery and Liver Transplantation and are actively involved in clinical research and offer multiple studies in areas such as hepatocellular carcinoma, gastroenterology and viral hepatitis.
For patients requiring hospitalization, we have a dedicated Hepatobiliary Critical Care Unit, a heptobiliary physician on call, anesthesia staff and a specialized OR nursing team. At the Center, our focus is on providing experienced, personalized care for all our patients.
Bariatric Surgery
We Care partner hospitals center for Gastroenterology & Hepatology performs Bariatric surgery as a specialized treatment for obesity. Bariatric surgery is performed if other forms of fat reduction methods like exercise or diet control do not produce the desired results. Bariatric surgery involves reducing the size of the stomach, leading to lesser food intake and gradual weight loss.
What is morbid obesity ?
Obesity is a condition in which one has too much body fat (adipose tissue). Obesity is determined by calculating the Body Mass Index (BMI), which measures weight for height and is stated in numbers.BMI = Weight (in kg).
Height (in m2)
BMI Status
Below 18.5
Underweight
18.5 - 24.9
Normal
25 - 29.9
Overweight
30 - 34.9
Obese
35 - 39.9
Severe Obesity
> 40
Morbid Obesity
> 50
Super morbid Obesity
Surgical options for treating Morbid Obesity
The morbidly obese have to seriously consider surgery for reducing weight to avoid its ill effects.
Surgery for Morbid Obesity is for the following situations : -
The persons BMI is over 40, or is 35 or higher and a serious medical problem (hypertension, diabetes, heart disease, joint problems, reflux) that is made worse by obesity is present
If it has not been possible to reduce or maintain weight under a medically supervised program
If the person has been obese for at least 5 years
Two surgical treatments are recommended for obesity : -
Gastric Banding : - Gastric Banding operations reduce the functional size of the stomach (with a gastric band, silastic ring or staples). This restricts the amount of food one can eat at one meal. By reduction of calorie intake, weight loss is induced.
Gastric Bypass : - Gastric Bypass procedures go further. This type of surgery helps reduce the amount of eaten food that can be absorbed in the digestive tract. So, not only does one consume less calories, but there is also less absorption of calories. This is why gastric bypass surgery tends to produce greater weight loss than other bariatric operations.
Hepatobiliary Center
With the use of advanced technology and surgical methods, patients now have more options than ever for the treatment of Hepatobiliary disease. We Care partner hospitals centre for Hepatobiliary surgery offers comprehensive specialty care for diseases of the liver, pancreas and bile duct.
For patients requiring hospitalization, we have a dedicated Hepatobiliary critical care unit, a heptobiliary physician on-call, anesthetists and a specialized O.R. nursing team. At the Liver Center, our focus is on providing experienced, personalized care for all our patients. Our doctors are trained at the world's most renowned centers in Hepatobiliary surgery and Liver Transplantation and are actively involved in clinical research.
Intensive training in areas such as management of hepatocellular and pancreatic carcinoma, viral hepatitis and new diagnostic and surgical capabilities have enabled the team to treat these disorders with the latest techniques.
Our team of surgeons, interventional endoscopists, radiologists and hepatologists work together to provide surgical treatment for the following disorders : -
Biliary
Carcinoma of the gallbladder
Malignant tumors of the bile duct
Bile duct injuries and strictures
Choledochal cysts
Recurrent pyogenic cholangitis
Pancreas
Pancreatitis
Pancreatic pseudocyst
Malignant neoplasms of the pancreas
Cystic neoplasms of the pancreas
Pancreatic islet cell tumors
Liver
Hepatic trauma
Metastatic neoplasms of the liver (Cancer originated elsewhere & spread to liver)
Benign (Non cancerous) tumors and cysts of the liver
Portal hypertension (portasystemic shunts)
With the use of laparoscopy and endoscopic ultrasound (EUS), all patients with malignancies are staged pre-operatively. Following staging, our Hepatobiliary team works in conjunction with the referring physician to determine the treatment best suited for the patient's condition.Since choosing a treatment plan is an important decision, we review all options with patients and family members as well as their referring physician, explaining the benefits and disadvantages of each option.
Liver Tumor treatment and Surgery in India
Biliary surgery is most frequently performed for stones, strictures and tumors. The treatment options available are : -
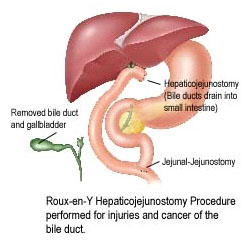
Resection of primary biliary neoplasms (cholangiocarcinoma)
Treatment of bile duct cancer usually requires removal of the bile duct and possibly portions of the liver, gallbladder, pancreas and small intestine. After resecting the neoplasms -- either through open surgery or laparoscopically -- the surgeon reconnects the bile ducts to the small intestine for proper biliary drainage (see illustration).
Biliary Drainage Procedures
Biliary drainage procedures are performed when the bile duct becomes blocked, narrowed or injured. During surgery, continuity of the biliary tree is usually re-established via a hepaticojejunostomy.
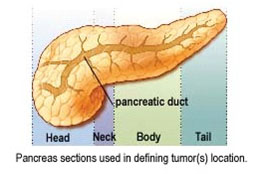
Managing diseases of the Pancreas
Upon referral of a suspected pancreatic pathology, the Liver Center's hepatobiliary team initiates a preoperative work up which usually includes an evaluation of pancreas via EUS. This evaluation helps to determine the location of the pathology in the head, neck, body or tail of the pancreas.
Subsequent treatment options include : -
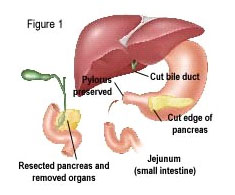
Pancreaticoduodenectomy (Whipple Procedure)
A pancreaticoduodenectomy, also known as a Whipple Procedure, involves the removal of the pancreas head due to a tumor in the pancreas or bile duct, or pancreatitis.
If a tumor exists in the head of the pancreas, it is usually necessary to remove the pancreas head, duodenum, gallbladder and a portion of the bile duct. Figure (1). Sometimes part of the stomach is also removed.
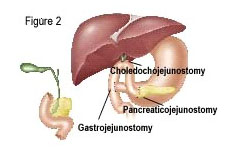
The end of a patient's bile duct and the remaining pancreas are then connected to the small bowel (Figure 2) to ensure flow of bile and enzymes into the intestines.
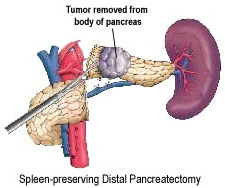
Distal Pancreatectomy (laparoscopic or open)
Indicated for tumors in the body and tail of the pancreas, a distal pancreatectomy involves the removal of cystic neoplasms either laparoscopically or with open surgery. With both laparoscopic and open distal pancreatectomy procedures, surgeons attempt to preserve the spleen.
Drainage Procedures
With chronic pancreatitis, a dilated pancreatic duct usually reflects obstruction.
Procedures to improve ductal drainage include : -
Longitudinal Pancreaticojejunostomy (Puestow Procedure) : - The pancreatic duct is opened from the tail to the head of the pancreas and attached to the small bowel.
Distal Pancreaticojejunostomy (Du Val Procedure) : - The pancreas is divided transversely at the neck, and the body and tail are drained via attachment to the small bowel.
Sphincteroplasty : - When endoscopic sphincterotomy is unsuccessful, surgical sphincteroplasty may be required of the minor or major papilla.
Managing Liver Cancer - Surgical Options
When determining treatment options for tumors of the liver, the hepatobiliary team reviews the results ofthe pre-operative evaluation and overall health of the patientto recommend appropriate treatment options. The majority of liver metastases come from the colon. The single tumor or even a situation where there is more than one tumor confined to either left or right side of the liver can be successfully resected with 5-year survival as high as 60%.
Treatments for tumors of the liver include : -
Surgical Resection (Tumor Removal) -- Open or Laparoscopic
Typically, surgeons can safely remove up to 70% of the liver (if there is no fibrosis) and expect full regeneration. During resection, the surgeon first uses ultrasound to determine the tumor's proximity to hepatic structures and then removes it with as little liver tissue as possible, while ensuring a margin free of tumor.
Portal Vein Embolization
For patients who may not have enough liver reserve, portal vein embolization is used pre-operatively. This technique, which involves the insertion of tiny microspheres into the portal vein, blocks blood flow to the portion of the liver containing tumor(s), and results in the enlargement of the remaining liver segments on which the patient will depend after resection.
Laproscopic Liver Resection
If the location of a benign tumor is superficial and small in size, the operation can be performed laparoscopically (by making small punctures in the abdomen while viewing through a video camera). We are one of the very few centers in South East Asia offering Laparoscopic Liver Resection.
Liver Transplantation
While a liver transplant represents the best cure for most patients with non-metastatic liver cancer, the limited organ supply may make this option unattainable. The eligibility criteria for transplantation is the presence of a single HCC tumor 5 cm. or less in diameter, or three or fewer tumor nodules, each 3 cm. or less in diameter. Both living-related and cadaveric liver transplants are options for patients at the Center for Liver Diseases & Transplantation, Apollo Hospitals.
Ablation (Radiofrequency or Cryoablation)
Patients who are not candidates for resection or transplantation due to inadequate liver reserve, large or multiple lesions in multiple lobes, fibrosis or cirrhosis can benefit from treatments such as CT-guided, laparoscopic or open radiofrequency or cryoablation.With new radiofrequency (RF) ablation technology, liver tumors up to 7 cm. in diameter can be treated. The ideal patient for RFA generally has no more than three lesions that are no greater than 5 cm. (about 1.5 inch) in size.
RF ablation delivers radiofrequency energy to the tumor, heating it to temperatures above 113 degrees Fahrenheit and thereby destroying the lesion. During cryoablation, argon gas is delivered through probes inserted into the liver, creating an ice ball that freezes the tumor and destroys its cells.
Percutaneous Ethanol Injection Therapy (PEIT)
Another option for patients who are not surgical candidates, PEIT involves the injection of alcohol into the tumor, causing immediate dehydration of the cytoplasm with consequent coagulation, necrosis and fibrous reaction. PEIT results in complete ablation in up to 75% of selected patients with hepatocellular carcinoma.
Hepatic Arterial Pumps
Indicated for patients with metastatic colon cancer, hepatic arterial pumps deliver chemotherapy to the liver through a catheter placed in the hepatic artery. The catheter is typically inserted via laparoscopic or open surgery and a pump, which delivers the chemotherapy, is implanted subcutaneously. The pump is generally filled with medication chemotherapy once a month.
Endoscopy
Endoscopy is routinely performed at the Center for Medical and Surgical Gastroenterology, We Care India partner hospitals in India for the following conditions:
For patients who suffer from gastrointestinal bleeding ,both Banding / injection of esophageal varices and control of bleeding with adrenaline injection / argon plasma coagulation are routinely performed.
For patients with swallowing difficulty due to esophageal stricture or achalasia, endoscopic dilatation can be carried out under fluoroscopic guidance. Similarly dilatation of pyloric and colonic strictures can also be carried out. In patients with esaphageal tumours, metallic stent placement is done, after dilatation.
For patients for whom feeding is a problem either due to neurological disorders or altered consciousness levels, endoscopic placement of nasojejunaltube or PEG (Percutaneous Endoscopic Gastrostomy) tube is done.
Endoscopic removal of gastric / colonic polyps is routinely done.
For patients with obstructive jaundice, ERCP / papillatomy / stone extraction from CBD/biliary stenting (plastic as well as metal stents) can be performed.
Placement of pancreatic stents in patients with severe pain due to chronic calcific pancreatitis is done.
Esophageal manometry, pH studies and rectal manometry, which are available in only limited centres, are done routinely and help not only in diagnosis, but also in deciding which patients with gastro-oesophageal reflux or achalasia are likely to require surgery.
Other routine procedures like liver biopsy, aspiration of liver abscess and diagnostic and therapeutic paracentesis are done through endoscopy.
The list of of Gastroenterology Hospitals in India is as follows : -
For more information, medical assessment and medical quote
send your detailed medical history and medical reports
as email attachment to
Email : - info@wecareindia.com
Call: +91 9029304141 (10 am. To 8 pm. IST)
(Only for international patients seeking treatment in India)
For a detailed evaluation send patients medical reports / X rays / doctors notes to info@wecareindia.com
Patient Storys
Successful heart surgery at We Care India partner hospital allows Robert Clarke to live a normal life despite a rare genetic disorder We Care india helped Robert find best super specialised surgeon for his rare conditions.
India Liver Disease, Endoscopy India, Gastroenterology India, Gastroenterology Hospital Kolkata, Gastroenterology Hospital India, Oesophago Gastro Duodenoscopy in Kolkata, Colonoscopy in Kolkata, ERCP in Kolkata, Oesophageal Manometry in Kolkata, Oesophageal PH Study in Kolkata, Rectal Manometry in Kolkata, India Liver Disease, Endoscopy India, Gastroenterology India, Liver Transplant India, Diseases Of Food Pipe Esophagus, Minimal Invasive Surgery, Endoscopy, Cholecystectomy, Appendectomy, Splenectomy, Tests For Hepatitis, Alcohol Problems, Ballon Treatment


 A pancreaticoduodenectomy, also known as a Whipple Procedure, involves the removal of the pancreas head due to a tumor in the pancreas or bile duct, or pancreatitis.
A pancreaticoduodenectomy, also known as a Whipple Procedure, involves the removal of the pancreas head due to a tumor in the pancreas or bile duct, or pancreatitis.