Cervical Spondylotic Myelopathy Requires Prompt Surgery
With widely varying signs and symptoms and no single pathognomonic finding, cervical spondylotic myelopathy presents a diagnostic challenge. Yet making the correct diagnosis is critical because appropriate surgical intervention is associated with improved outcomes.
Cervical spondylotic myelopathy, the result of narrowing of the cervical spinal canal by degenerative and congenital changes, is the most common type of spinal cord dysfunction in patients older than 55 years and the most common cause of acquired spastic paresis in the middle and later years of life.
Pathologic mechanisms
Both static and dynamic mechanisms are involved in the pathogenesis of cervical spondylotic myelopathy. Static factors include congenital spinal canal stenosis (<13 mm anterior-posterior diameter); disc herniation; osteophyte formation in the vertebral bodies; degenerative osteophytosis of uncovertebral and facet joints; hypertrophy ligamentum flavum posterior longitudinal ligaments.
Dynamic factors are abnormal forces placed on the spinal column and spinal cord during flexion and extension of the cervical spine under normal physiologic loads. Trauma caused to the spinal cord by repetitive compression against an osteophytic bar during normal flexion and extension of the cervical spine is an example.
C5 through C7, the region of the spine with the highest frequency of cervical spondylotic changes, also is the area in which the vascular supply is the most tenuous.
Cervical spondylotic myelopathy can also be caused by spinal cord ischemia. Pathologic findings that indicate a vascular mechanism include spinal cord necrosis and cavitation in gray matter.
Insidious onset
The onset of cervical spondylotic myelopathy is generally insidious, with long periods of fixed disability and episodic worsening. In one series, symptom duration ranged from one week to 26 years. Almost half of patients presented with symptoms of more than one year in duration.
Cervical spondylotic myelopathy causes a variety of signs and symptoms, and has no single pathognomonic finding. The first sign is commonly gait spasticity, followed by upper extremity numbness and loss of fine motor control in the hands.
Other symptoms : -
Pain in the neck, subscapular area or shoulder.
Numbness or paresthesia in the upper extremities, usually nonspecific.
Sensory changes in the lower extremities.
Motor weakness in the extremities.
Gait difficulties ("spastic gait," hesitant and jerky).
Myelopathic or "upper motor neuron" findings such as spasticity, hyperreflexia, clonus, Babinski and Hoffman signs, and bowel and bladder dysfunction.
"Lower motor neuron" findings such as upper extremity hyporeflexia and atrophy.
Diagnosis
The differential diagnosis of cervical spondylotic myelopathy is quite broad. It is important to rule out multiple sclerosis and amyotrophic lateral sclerosis. Cervical spondylotic myelopathy does not affect the cranial nerves or the normal jaw jerk reflex, whereas the other disorders may. In addition, amyotrophic lateral sclerosis is a pure motor disease, therefore, sensation is unaffected. Cervical spondylotic myelopathy may have motor findings similar to those of amyotrophic lateral sclerosis, in addition to sensory findings such as numbness or paresthesia in the upper extremities.
Other disorders in the differential diagnosis include spinal cord tumors, syringomyelia, subacute combined degeneration, cerebral hemisphere disease, and peripheral neuropathy. Normal pressure hydrocephalus, which may have gait and bladder involvement, should also be considered.
Radiographic studies
The diagnostic workup of cervical spondylotic myelopathy often includes cervical radiographs, which may demonstrate osteophyte formation, kyphosis or subluxation. The most valuable tool, however, is MRI. Along with the ability to rule out a tumor or syrinx (a slit-like cavity in the spinal cord), MRI permits specific evaluation of the spinal cord, intervertebral discs, vertebral osteophytes and ligaments.
Surgery
Cervical spondylotic myelopathy patients treated medically (i.e., with collar immobilization and traction) show continual progressive neurologic deterioration. One series of 1,355 patients treated conservatively revealed no improvement in 64 percent and neurological deterioration in 26 percent.
In addition, patients with cervical spondylotic myelopathy are at an increased risk of spinal cord injury from relatively mild trauma.With decreased anterior-posterior diameter of the cervical spinal canal, the spinal cord has limited room to move. Many traumatic cervical injuries are due to hyperextension, which results in maximal narrowing of the spinal canal.
Early surgery can improve prognosis. Montgomery and Brower found that the prognosis after surgery was better for patients with less than one year of symptoms, young age, fewer levels of involvement and unilateral motor deficit.
Dorsal or ventral approach ?
Both dorsal and ventral surgical approaches are appropriate for cervical spondylotic myelopathy. Since no clinical study has demonstrated a significant difference in the outcomes of the two approaches, the choice is based on surgeon preference.
The dorsal approach involves cervical laminectomy, while the ventral approach involves either discectomy at one or more levels with interbody fusion or one or more corpectomies with interbody fusion. Corpectomy typically involves cervical plating to provide stability until fusion occurs.
Factors guiding the surgeon's decision : -
The relative location of the stenosis (dorsal vs. ventral) : - For patients with cervical spine stenosis that primarily results from dorsal compression, cervical laminectomy (dorsal approach) is better. For patients with ventral disc herniations and osteophytes, however, cervical laminectomy alone does not allow sufficient access to the ventral spinal cord. These patients may benefit more from a ventral decompression and fusion procedure.
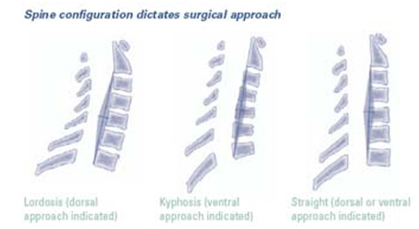
The alignment of the cervical spine (kyphosis vs. lordosis) : - For patients with effective cervical kyphosis, dorsal decompression is associated with a high probability of failure. In these patients, cervical laminectomy can worsen the ventral spinal cord compression by tethering the dural sac and its contents over ventral osteophytes, which leads to neurologic deterioration. A dorsal approach in this situation may also lead to progressive kyphotic deformity and instability requiring repeat surgery and stabilization.
For patients with effective lordosis, a dorsal approach is often optimal for spinal cord decompression, especially with dorsal compression. It should be noted that when compression is ventral (e.g., herniated nucleus pulposus), the decompression is optimally performed from a ventral approach, even if the cervical spine is configured in lordosis.
Between kyphosis and lordosis is a "gray zone" in which the surgical approach is chosen on the basis of the biases and clinical judgment of the surgeon
The list of of world class Spine hospitals in India is as follows : -
For more information, medical assessment and medical quote
send your detailed medical history and medical reports
as email attachment to
Email : - info@wecareindia.com
Call: +91 9029304141 (10 am. To 8 pm. IST)
(Only for international patients seeking treatment in India)
For a detailed evaluation send patient’s medical reports / X rays / doctors notes to info@wecareindia.com
Patient Storys
Successful heart surgery at We Care India partner hospital allows Robert Clarke to live a normal life despite a rare genetic disorder We Care india helped Robert find best super specialised surgeon for his rare conditions.